Cardiologist and echocardiographer Nisha I. Parikh, MD, MPH, discusses acute and chronic cardiovascular issues in COVID patients, and how imaging can help with early diagnosis and monitoring treatment response. She also looks at the consequences of delayed care for heart events due to patients’ pandemic-related anxiety.
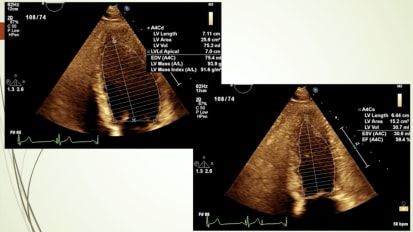
Mm. Mhm. So, in terms of objectives, therefore, for the talk, I want to review a little bit of the current epidemiology of covid 19 in the United States and locally also wanted to review some considerations of vaccine. Um, since that's sort of on everyone's mind right now and also, uh, then go into the cardiac manifestations in covid. 19 in the acute illness, reviewing some of the biology and path of physiology and why there would be links between COVID 19 and and the heart and then also review some chronic cardiovascular considerations with and then throughout the talk. I have a lot of imaging correlation. So I'll just for folks that aren't as familiar with, for instance, echocardiograms and such, Um, if you if you don't see it in your line of work, then I'll just review that a little bit. So bear with me if you are very familiar with those, um, so in terms of thinking about the pandemic, currently, this is really current data for the United States and for California. So in the Bay Area, we've had, uh, as of essentially, um, Jan 21st, we've had 349,000 cases and unfortunately, 35 100 deaths. And in California, we today just past three million cases for the first time. And I think that might be the high, uh, in the United States in terms of state and unfortunately, 35,000 deaths. Of course, in the United States, the numbers are pretty staggering at 24 million cases and now we've passed 400,000 deaths. This graphic just sort of reminds us what where we started and where we are. So this is sort of a depiction of cases from march to today and so you can see that the pandemic largely started on the coasts. And as you get darker red and purple, you sort of have more cases within each county. And, you know, if you're sort of looking today really, that Midwest sections filled in quite a bit And, um, covid is essentially almost everywhere and California in particular. If you look, um, we have certainly lots of purple in the major metropolitan areas of California, really only red and light red, light red in the in the pretty, sparsely populated areas of California. Um, I want to talk a little bit about vaccine rollout. Um, and I know that this, um certainly, uh, your your group encompasses both Alameda and Contra Costa County. So I pulled data from both of both of these counties. I actually live in Contra Costa County. So near and dear to my heart, even though I work in San Francisco. So, in terms of Alameda County, this is this is actually our vaccine numbers. So this is total doses doses administered per 100,000 people, with the lighter blue being closer to zero and the darker teal here being, um uh, 5000, uh, for the 100,000 population so you could see definitely along the coast. Um, you know, we sort of have the the more doses administered in Alameda County. Um, there have been, um uh, 300,000. Uh, 33 100,000, um, or 35? Uh, I'm gonna say it wrong. Well, you get the picture. You can read this number here. Uh, doses administered. So about almost 5000 doses for every 100,000 people 16 and older in Contra Costa County. The numbers are actually I don't know why it's it says the exact same number. That's a little bit curious, so that didn't work. Um, but in any case, I know the Alameda number was accurate. So apologies for the Contra Costa. Um, issue. I want to talk a little bit about the effectiveness of the vaccine. And this might be a review for a lot of folks. Um, but just to kind of remind us in the context of other vaccines that have been around for a while. So the influence of vaccine has an effectiveness of 44% and I think oftentimes we forget about that low number. Of course, you only really need one for the most part of the flu vaccine. Although I know in some populations, um, there there might be more than one does. The AstraZeneca vaccine hasn't really been as widespread use in the United States, but that has about a 70% um, effectiveness. You need two doses of that. Chicken pox is more effective than the AstraZeneca coronavirus vaccine, and that has a 92% efficacy with two doses. Moderna and Pfizer are really the vaccines that, um that have been, um, administered in California and around the United States. And they have a 94 and 95% effectiveness with two doses each. And if you compare these, um uh, in terms of thinking about the type of vaccine, the AstraZeneca vaccine is a vaccine that we have sort of used in terms of the paradigm of the vaccine. So it's a genetically modified virus. It's basically an attenuated coronavirus, um, and the actual virus And, you know, the the the effectiveness, however, of that approaches is not quite as high as Madonna. Revise ER, and it is important to note, sort of, um, one advantage of that vaccine is that you can have it at regular bridge temperature. And if you compare that with the Madonna and the Pfizer Bio n Tek vaccine, those are are in a vaccines, and these are a new technology we haven't really used before. Um, in this in this sort of wide spread population paradigm, and basically they have taken part of the virus genetic code, and I think in particular they taken a spike protein are any and that essentially is translated once it's injected back into the protein and then the your your body creates antibodies against that two doses each high efficacy as we as we mentioned. And the Madonna needs to be started Negative. 20 degrees Celsius. And cannot the dose once sort of, uh, sent out can last up to six months. The Pfizer biontech has to be stored at negative 70 degrees Celsius, so a little bit more complicated. And then we were not most likely going to use this, But, Nick, um, five. But this is sort of information for that one. So, um all right. So how effective? You know, what did the data look like? That that caused the FDA to to approve these rather quickly for by Pfizer biontech this I pulled just directly off the f d a, uh, memorandum that approved the vaccine, and this is sort of hard to read, But essentially, Day zero, you know, this was given to placebo and to the intervention group, the vaccine group and the vaccine group. This is the cumulative incidence curve for the first covid 19 occurrence after the after dose one. Um, and this is the efficacy. So this is basically the red is placebo. So you could see that they started developing covid. Um, about seven days after the first dose was given or actually right away. Really? They you know. So I think what this shows you in the blue is the vaccinated group. And so seven days after the first dose, either placebo or the vaccine, the curves are sort of similar because I think, you know, our our own bodies hadn't made their bodies. Hadn't made the antibodies yet after that first dose within a week. But after the week, you can see immediately that these curves start separating and that this vaccine is actually pretty effective. Very flat rates of covid 19. And if you want to look at the raw data, basically overall, nine people who received the Pfizer vaccine got as what they called serious covid 19 and 169 within the placebo got covid 19. When they calculated the efficacy rate, it was 95 almost 95%. It is also important to note that none of the people who who got vaccinated with this vaccine actually died of covid and you can see the rates broken down by age group and from Moderna. The results are pretty similar, with the curves separating at about 10 days. Maybe it takes just slightly longer or, you know, if we went back and looked at that. But I think you have to assume after the first dose, um, in about a week, you'll see a difference, Um, in in efficacy between the placebo and the the vaccine group. And here you could see that they vaccinated. Uh, about 26/27 2800 folks. And the vaccine and placebo group 11 within the vaccine group got, um, covid 19 that they considered serious and 185 within the placebo group. The other thing to note is that none of the folks that got COVID 19 within the vaccine group, I believe none of them were on supplemental oxygen. So the covid 19 that they got was actually less less serious. All right, so that's kind of a just a review of of vaccines. Um, you know, I kind of was just going to speak where we are in terms of California and vaccinations. And really, it's things that you probably are aware of. Two. It's mostly things that I get off the news, which is that our vaccination, uh, sort of rates have been relatively low compared to the rest of the country, unfortunately, and also that potentially, we haven't been as well organized in our vaccination efforts, and or maybe we just haven't received as many vaccines. It's hard to know. Maybe we'll know more when they are clears when you know, sometimes gone by. Um, now I wanted to shift gears a little bit and talk about Covid 19 longitudinal, uh, cardiovascular effects. And if it's okay, I might just answer questions at the end. I hope that's okay, but I do see that there might be some in the Q and A so I definitely recognize them. Um, so thinking about the longitudinal cardiovascular effects a covid 19. I want to talk a little bit first about the acute infection and how. How covid 19 immediately sort of, um, is part of the cardiovascular. PETA physiologic pathways in the receptor that it attaches to talk a little bit about acute illness and the potential for myocardial injury endothelial injury and also hypercritical ability in covid 19 1 to touch upon this really important issue of chronic illness, the so called long haulers that many of you probably see, uh, that present with, um, several symptoms that are cardiovascular in nature as well as other symptoms, of course. And then I wanted to talk about some of these meta effects. I call them better effects of the pandemic that lead to delayed care, late acute myocardial infarction, presentation and even stress cardiomyopathy. Um, that we've seen as a result of of some of the emotional component of the pandemic. Mhm. So, um, sorry is Kobe to the virus that causes covid 19 enters the cells through the ace two receptor. And these two is the angiotensin two receptor, its receptor that is similar to the ace one receptor, uh, in sort of in a counterbalance pathway, the ace one receptor being the one that we think of as the target race inhibitors. So, ace, too, I think of as almost like the yin and the yang. Um, so it's the opposite sort of thing with ace one. You know, we're sort of trying to block that pathway and block the green, an angiotensin valdosta phone system with all of our therapeutics that are geared towards, uh, towards hypertension and also heart failure. Now, with the ace two pathway, it's actually the counterbalance to that pathway. So, um, with the ace two pathway. The downstream effects are essentially very beneficial. And they include, um uh, visa dilation. Um, uh, it's sort of antibiotic effects on the heart and the vasculature. And so, um, immediately when we we sort of recognize that starts Kobe to attach us to the ace Two receptors. And that's how it gets into cells. I think a lot of cardiologists were immediately sort of intrigued. Like, Wow, we've never really had a major sort of respiratory infection that that were, You know, that's been this widespread that that preferentially binds to a cardiovascular. Um receptor. So we wondered initially, You know what? What? That could mean. A stew, of course, is found in the lungs, Um, for sure, but also in the heart and blood vessels as well. And the kidneys. So another interesting feature of this disease, which you know, I think we haven't quite sorted out Why, um is that there are many cardiovascular comorbidities that puts a person at risk for serious covid 19, um, including diabetes and hypertension. Um, and also obesity. To a certain extent, that lead to sort of a more serious manifestation of covid 19. But the thing that's curious is that you don't really see this in other causes of a R. D s and other respiratory illnesses like influenza. In fact, diabetes and hypertension aren't really risk factors for influenza. Um, so it's sort of curiosity, um, that that these to put a person at risk for covid 19. And we wonder if, um, the role of the H two receptor might be involved in in this, um, epidemiology that we see. And in this study, which was from many provinces and excuse me, hospitals in China, Um, this group noted that if somebody had two or more of those comorbidities on the slide before that, they had a higher, um, higher rate of adverse outcome, including admission to the ICU. Invasive ventilation or death. So, um, switching gears a little bit, um, we, you know, sort of recognized early on that there might be the rule. Um, there might, that there are. There is, in fact, cardio vascular involvement in covid 19. That might be, you know, due to to some of these links that I mentioned and, um, so So I'm going to present some cases that include eco findings, um, that help us sort of diagnose some of these cardiovascular conditions. These can include, uh, these can include Ah and Anna Anna. Body related cytokine storm from a serves like illness. And this can involve, um, disseminated intravascular coagulation occlusion in the micro vasculature of the heart. And also in the micro vasculature and macro vasculature of the lung. So, um, pulmonary embolism is seen. Um, there's also the manifestation of a respiratory induced hypoxia mia, and that can cause our right ventricular strain and dilation, you know, sort of seeing seeing all of that. Um, all of that sort of lung pathology can sort of back up onto the right side of the heart, and you can get right sided heart failure, and then sars-cov-2 can actually also directly infect the heart, but probably by the ace two receptor get into the myocardial, and this can cause a myocarditis. So my signal, Croesus and and you and and sort of a more kind of severe myocarditis like picture. And you can see some of those cases. Um, so the echo can help with early diagnosis, risk stratification, human dynamic monitoring, and also assess the response to treatment. So, in terms of echocardiograms in Covid. 19. This is a case series from I think this was either Mount Signer Cornell in New York. They had 100 consecutive patients with Covid 19 who had complete echoes within 24 hours of the admission during the sort of large surge right at the beginning of the pandemic in the United States. Uh, and these were compared to reference echocardiogram. So people that were sort of like age matched co morbidity matched, if you will. And they found that on 39% of the echoes there was RV dilation or dysfunction. 32 had a normal eco. Uh, there was LV, diastolic dysfunction in 16% of folks and 10% had LV dysfunction, with 3% having valvular disease. So that's kind of the breakdown of what you'd see if you were to get an echo in someone who you suspect that might might need one. For those reasons we went over, Um, you can see a sudden decline in systolic function on the Doppler, and that's what this shows that might be getting a bit too technical. But you could see on this bottom picture here that this is how we measure stroke volume on an echo. It's the L V um, volume time integral of the flow across the left ventricle. And you can see it's blunted Here. Um, so here's baselining. Here's two days later. So there's other things besides just looking at the picture of the echo that helps us. Um, so how how does stars, we, uh, Kobe to cause, uh, cardiac dysfunction? It can be the stress of the a R. D s itself. Uh, the immune response caused by a micro Davis. And so it's not really sort of like a direct infection, but the immune response to an infection or direct infection. And there's actually now biologic data that support all of these things. Um, mhm. We, um And I think I I mentioned that, um, that you know, the biologic data. So when you look at human, um, stem cells, uh, and sort of a cardio Maya sites. And in a dish, you sort of have the virus infect these cardio Maya sites. Um, they stopped. They and, um, they cluster basically in the peri nuclear region where the viral particles are produced. You can see that with the arrows that they cluster in those regions. And, um uh, and so that's some evidence of infection. Um, the the EPO itself. Um, And it Excuse me, Um, some of our data on cardiac, I should say strain, um, vis a vis, uh, these biomarkers of cardiac troponin and myoglobin in in Chinese. Uh, longitudinal cohort actually predicted sort of a worse outcome. So you had a patient with an elevated troponin. You know, you want to take that person a bit more Seriously, um, if they if they have covid 19, because that did predict a worse outcome. Um, this is a case from UCSF. This was our first cardiac case, uh, with a patient had covid 19. And it was an elderly gentleman who presented with who had a history of chronic atrial fibrillation and heart failure with preserved ejection fraction, who had a recently treated mitral valve endocarditis. Um, and he was sort of recovering from that, um, in a sniff, but was admitted for shortness of breath, coughing, chest pain, um, a federal at the time. So he was He was just admitted to the regular cardiology service, and this was his chest X ray with bilateral infiltrates. Um, you know, sort of heiler infiltrates concerning for heart failure. He had crackles and pitting oedema and his e k g showed a fib with RVR. Um, he was given some ivy diuretics. Admitted to cardiology for acutely compensated heart failure. Um, and he became somewhat hypertensive. So Dorothy was started. Um, he did subsequently have, um, SARS cov two RNA test. That was positive, Um, so later was sort of transferred to to a to the to the covid unit. His echo showed an LV of 70%. And although he was given, um, Diaries A stays, oppressors, arts net ventilation, his respiratory, um, status decompensate. And unfortunately, um, his family eventually declined. Sort of, um, stepping up treatment. Um, and so he was transitioned to d N R D N A, uh, Died on hospital day seven. So that was an example of Sort of acute on chronic heart failure. Um, decompensating heart failure as a manifestation of covid 19. This is a case of covid 19 myocarditis. So this is another case from UCSF. This is a 69. Oh, excuse me. Not from UCSF. This is from, um I actually got this from the literature. This is a 69 year old man who was admitted to the ICU for covid 19 a r. D. S. You can see that in his lung here. His lung, uh, his c t of his chest. Excuse me, was put on mechanical ventilation is troponin was elevated. He was taken to the cattle, but found to abnormal grown aires. And this was his e k g. Just showing, um, l ve h with some t wave inversions across the creek. Cardio lead. Um, he had an echo, which again I sort of got from the land set. And, um, this showed a normal, uh, initially, um, but he also had a CMR, and this showed, um, delayed enhancement of the infra lateral wall that was suggestive of my credit is So that's sort of where this arrow is pointing. It sort of lighter, uh, than than, um, the regular sort of like dark, darker, myocardial in the septum. He was given nine days of Hydrocortisone zone, spent three weeks in the hospital and discharged home. So, um, he had myocarditis with sort of, you know, without, like, a classically severely reduced. Yeah. Um, this is another case of myocarditis again from the literature. We haven't really seen too much of this at UCSF, which is why I pulled these from the literature. But this was a 15 year old boy admitted with chest pain and a mild fever, a CRP of 41 in a troponin that peaked at 13. The chest CT was within normal limits. And this is his e k g, which basically shows Sinus rhythm and just sort of non specific changes. Maybe a little bit of peaked peaked t waves in the Precor diem, but nothing really to speak up. And this younger boy, this is some of his echo, which shows a mildly reduced ejection fraction. This is the para sternal long access just to remind you, um, so this is the left ventricle and the right ventricle, and this is kind of going through a few different views quickly, so I can back it up a little bit, but But you can see that there's sort of a mildly reduced ejection fraction here. And that's, you know, kind of on my qualitative view of this echo. All right. Okay. Um, this boy also had a cardiac MRI, and, um, he had a sort of diffuse, uh, inflammation that you could see on on this, uh, image here? A It's Yeah, Postrel lateral inflammation here. Although it sort of looks diffused to me with white all over the medium. Um, and he had late Catalonian enhancement in the in for a lateral area. And that's this, this white section right here. And see indeed that you could see. So he had he had an episode of essentially myocarditis. Um, here was, uh here was a another separate article. This is different now that shows some path of pathology. Um, that that basically of covid 19 myocardial tissue. Um, and pathology. Basically, this shows that you can see a lymphocytic infiltration. And you can also see interstitial macrophages when you look at the, uh, pathology of the heart and covid night to myocarditis. Um, so in conclusion, you can have either a normal, uh, normal or a low normal L V E f. Uh, pericardial effusions can also be seen. And, um, uh, you know, I think one of those MRIs had a little infusion. This can be multi system or isolated. You can have a relatively rapid recovery. Um, and cardiac MRI can be complementary to, um, to trans thoracic echo. And certainly, if you have elevated biomarkers, chest pain in kg changes and you're suspecting it, you can certainly order uh, mari just to confirm that diagnosis. Um, in terms of the right ventricular parameters, this is sort of more technical stuff, but But we have ways now in the modern echocardiogram where we can really get a more accurate size of the right ventricle and also function. And so some of those technicalities were on that slide. I'm not going to belabor those, um, there. Why is that important in covid 19? Well, this data, basically again from from a Chinese cohort showed us that, um that if you if you look at the lowest middle and highest turtle of patients with with what we call our V longitudinal strain a measure of our RV dysfunction, um, those patients had essentially sort of like these graded risks, um, in survival, uh, free of of, um, of mortality and serious outcomes so that if you had worse RV function, that kind of predicted or worse outcome, it's sort of, you know, a little bit logical, because they probably also have worse, uh, lung function as well, but But the RV can be prognostic. Basically, in covid 19. This is a case from a colleague of mine in New York who, right at the beginning of the pandemic, she's nice. You doc there had sent me this echo in the middle of the night and just kind of, you know, in the middle of all of everything, she was just texting, getting like a curbside consult. So this was her. Her point of care. Ultrasound. Basically, um, this is a patient with hypoxia, hypertension. Um, and it shows a very sort of flattened left ventricle. Um, that is somewhat under filled. And the right ventricle is really all up here. We can't even see the edges of it. So, um, certainly in this patient with hypertension hypoxia, this was, um, right. Ventricular failure. And, you know, relatively under filled LV. Might want to give this patient some fluids. Um oh, come to the next, um, next slide here. I think I might skip this one. All right. So, uh oh, actually, was there a good point here? Well, the only point I want to make here is that, um, in that covid 19 pneumonia. If someone becomes more hypoxic or they're having sort of classic symptoms. Pulmonary embolus is something you should think of, and this isn't really the perfect example of it, but this person does have a pulmonary embolism. They have some flattening of their septum, which is really some pressure. Um, overload of the absolute, um, right ventricle. So, um, why is this? Well, um, the respect this is really, um, due to, um, kind of workhouse triad. So? So there is an acute illness. Um, folks are obviously sedentary, bedridden? Um, and there is inflammation, um, and material dysfunction on that basis, um, and most, uh, static abnormalities can result the clinical outcomes of this hypercritical ability and covid 19 include, um, venous thrombosis, embolism, myocardial infarction or D I. C. Um, there are some guidelines for covid 19, um, and basically stayed the same That these that predisposes to arterial and venous thrombosis. Initial series suggested the common occurrence of DTE and patients with severe covid 19. The optimal preventive strategy is a little bit unclear at this point. Um, basically, uh, you know, the guidelines from this is from a while ago now suggests that the available technology should be used to optimally care for patients, um, with covid 19 that have robotic disease throughout the pandemic. But I think that although some trials have been done, it's still a little bit unclear. Um, in the inpatient setting, you know who you need to anti coagulate and if it should be with prophylactic or therapeutic anti coagulation, Um, and also what to do in the outpatient setting. Some people would actually give antique regulation, even in patients and out in the outpatient setting, depending on some of their other risk factors. Wanted to switch gears a little bit to talk about the chronic cardiovascular effects of covid. And, um, these can include sort of symptoms in the so called long haul patients, including palpitations, tachycardia, um, dizziness, precinct API, Disney on exertion and chest pain. Um, this is, uh, an echo in a patient that had, uh, the long haul symptoms there was sort of like, uh, you know, normal to low normal ejection fraction. The global longitudinal strain, however, was slightly reduced at negative 16%. Strain is just a marker of left ventricular dysfunction that we sometimes get. Um, that can be like a early marker of LV dysfunction. Or it could just be something subclinical that doesn't really develop. And in this case, the right ventricle was slightly enlarged as well. For the most part, the echoes I've gotten in folks that have long haul covid symptoms are normal. That's really the most frequent kind of echo that I've seen. Thankfully, um, uh, we have seen low normal ejection fraction. This is an example of a low normal ejection fraction of 50 to 55%. Um, there have also been studies looking at cardiac MRI following covid 19. Um, this this study looked at 50 healthy volunteers and then risk factor match patients. Um, and the healthy volunteers had had covid 19 before, but had been relatively, you know, well recovered, um, 67 recovered at home. 33 required hospitalization. Um, and at the time of the cardiac MRI, high sensitivity troponin was detectable in 70. Um, one. Excuse me. And, uh, see, you need, um, in in many of the patients. And there was myocardial inflammation and scar seen in, um, in sort of a majority of patients that had had covid 19. But, you know, I have to say that 78% of the patients. Uh, with with covid 19, I have to say that we There's a lot of skepticism by most in the cardiology field that these results actually can be extrapolated to the general population. So that is to say that, you know, there haven't been that many studies that have been able to replicate this finding, Um, so I sort of take it a little bit with a grain of salt. Um, at this point, um, pericarditis is also another manifestation of covid 19. And I think we already talked about this clinical LV dysfunction. So what's the take home point in a long haul patient with symptoms if you're really concerned, Um, you know, and echoes are reasonable for starting point with the palpitations. I've gotten holter monitors. If the symptoms are sort of, you know, frequent enough or zio patch is, um just to make sure that they aren't having inappropriate Sinus tachycardia or other arrhythmias. Um, you can also, if folks are, like, really nervous to exercise, you can put them on a treadmill and sort of see how they do in terms of their, um, their response to exercise and that can provide reassurance for them, or it can kind of confirm that they are having this inappropriate Tecca Cardia. Very rarely. We have seen heart block in patients post covid young patients, otherwise healthy, structurally normal hearts. Um, and then finally, um, if if you sort of really also want to get at this issue of scar you, no one could consider a cardiac tomorrow as well. Um, if you know, if you felt that it was clinically indicated, wanted to switch gears a little bit. Now talk a little bit about the meta effects of covid 19. Um, initially in the pandemic, we we actually saw a reduction in the activations for STL elevation M eyes across the United States. So this was data from January of 2000 and 18. Um, and if you sort of looked, um, January of 2020 things were looking Okay, um, and then you see this sort of drop off if you compared to the year before, Here's March 2018. And here is March 2020. And so we sort of wondered what was going on. Where had all these stem ease gone? Um, and if you look at Northern California data. This is data from Kaiser, Northern California. There was a decrease in acute my activation during the covid period. Um, you can see that here, Um, as Kobe 19 rates rose here in the blue, you had a decrease in acute M I hear in the darker red 2020. Um, what are the implications of this? And what? You know, what other things to think about. So this was a recent case, Um, and this is sort of more of like the implication of, like, a delay in care. So there's a 52 year old man with no no medical history, several days of shortness of breath, chest pain, and back and shoulder pain who didn't seek care because he thought it could be covid. But he was then encouraged by his mother, um, to seek care. So he called EMS. This was his EKGs. I can see that. He has, um, these s t elevations in 23 and a via so in the inferior leads. And he also has t wave inversions that are sort of what we call reciprocal. And the lateral leads here in one and a V l and also interior early in B two Mm. A steamy code was activated. A stormy was activated. He was taken to the cath lab and found to have the inclusion of the R C. A PC. I was done on the R c. A. And, uh, an echo basically showed hypoxic genesis of the inferior wall of the left ventricle. Um, he continued to have chest pain, however, and what this shows you is it's not very evident. Um, you know, even to somebody looking at the echo who reads echoes. But But what you do see is you see, this is the left ventricle here. This is the left atrium and the mitral valve. The aortic valve sits over here in the ascending aorta is in this area. What you see is you see this this sort of Doppler flow, which is blood flow in the left ventricle. And what's unusual is you're seeing this flow, uh, systolic flow also in the right ventricle, which shouldn't be there. Um, so that sort of tips you off to the fact that oh, boy, here's a gentleman who came a bit late, um, for his steamy and he has this flow in the right ventricle. Could this gentleman have mechanical complication of an M? I, um, And indeed that is what he had. He had a ventricular septal defect. And what you can see is that in the sub costal view, which we do sort of underneath the disease avoid You can see that there's this discontinuity between the septum here, so you can see that here. This is the left ventricle, and this is the right ventricle. And so this gentleman, unfortunately, suffered a VSD, and you can see that flow here, that communication between the two ventricles. And that's something we used to see more commonly. Um, in the in the era before, we actually did short portable in times and such. So he had a mechanical complication, which is pretty rare. Now, we don't see this that often. Um uh, Let's see here. Um okay, this is just another sort of similar case and of of sort of a late presentation of an M. I and this gentleman had a whole systolic murmur following his revascularization for M I, and he had another mechanical complication of an M I around this time when folks were like staying home in delaying care, and that was a rupture of the papillary muscle. So this is sort of a now upside down from a trans thoracic echo. This is the left atrium, the mitral valve. Um, and this is the left ventricle. This is the Kordell apparatus of the mitral valve. So the mitral valve you remember attaches with cord tendon a two papillary muscles. And that's sort of how this beautiful structure operates in all of us. And you can see this jiggling, uh, glow mass here. And that's the papillary muscle, unfortunately, ruptured and causing severe mitral regurgitation, which you can see here, this sort of mosaic color jet coming back into the left atrium, that sort of severe regurgitation from that mechanical complication. So there definitely are are really unfortunate sort of consequences of these delays in care. And I think some of these are meta effects of covid 19. Unfortunately, this is a woman with chest pain, hypertension, 76 year old woman who I took care of over. Um, this must have been about three months ago. Four months ago, um, and she she essentially had a talk at pseudo cardiomyopathy. So she has this sort of ballooning of her left ventricle. For those of you haven't heard of that, it's also called stress cardiomyopathy or broken heart syndrome. And for some reason that when I was on service and this might just be anecdotal thing, I had to women with the stress cardiomyopathy and both of them describe, you know, just sort of severe stress of being at home alone. And maybe some things had happened to family members, maybe covid related or other health conditions. And, um, I think that acute psychological stress had led to this really sort of, you know, definitely real condition of stress. Cardiomyopathy is kind of a classic case. It's called Takatsu bo cardiomyopathy because in first noted in Japan and to Kosovo is the Octopus vessel. It's a It's a jar in which fishermen used to or, you know, catch octopus, and it's sort of like a wide white jar to catch the octopus. And that's sort of what the left ventricle, unfortunately looks like. Um, so she she was taken her Ikea jihadist Emmy pattern, Um, which is classic in this condition. She was taken to the cath lab, and her coronary arteries were clean. Um, so I just wanted to, um, to sort of, um I can skip that. So she had she had stress cardiomyopathy. Good news with stress cardiomyopathy. It has a pretty good prognosis if you sort of get them through that acute phase. Although sometimes it can be quite severe. They might even need ICU admission for a short while. I have had people also, um, you know, sort of have really serious arrhythmias in this condition, But if you get them through that, get them on sort of optimal medical therapy. Usually the LV will recover. Um, so late in these cases of, uh, acute myocardial infarction. Want to remember mechanical complications? Um, and these are just some technical sort of echo echo features that we like to think about. I'm going to skip over that. I had already talked about a case of covid 19 and a R. D s. So, in conclusion, um, I think there are a lot of connections between covid 19 and cardiovascular disease, including the acute infections. So we sort of went over a path of physiology. Um, we talked about acute illness. Um, manifestations there. This can result in a left ventricular cardiomyopathy that can really have a normal, uh, ejection fraction or even sometimes reduced, um, and right ventricular dysfunction from, uh, from a R D s or from a pulmonary embolism. Those are the two things to keep in mind. The chronic illness has a lot of symptoms that are cardiovascular in nature. And sometimes on eco, we see a borderline ejection fraction or late gadolinium enhancement, which is indicative of a scar on cardiac MRI. Um, and also all those other tests that I mentioned can be gotten. So, Holter, monitoring our zio patch, um, stress testing is reasonable. Um, and certainly an e k g. You can start with simple things like that to, uh, in terms of the pandemic what I call meta effects. There have been delays in care late AM my presentation and also stress cardiomyopathy, um, that we've seen. So keep those in mind. Um, and you know, to take those complaints seriously in our patients that sometimes aren't taking as good care of themselves are seeking care as much as they should. And hopefully some of that's changed a little bit. Uh, wanted to acknowledge some of my colleagues here on the slide. Ted Abrahams, the director of our Ecolab police fosters and emeritus faculty member whose colleague of mine pushing Sony is one of my colleagues, is the interventional cardiologist, and and he provided a lot of the cap cases that he had seen for me for this talk. Bruce Conklin is a basic science calling at the at the Gladstone, and he's had a lot of insight into some of these myocarditis connections on the molecular level, and Greg Johnson and Ben Kellman, or two of our cardiology fellows who've done, you know, really a nice job of of collaborating on some of these talks with us.
Related Presenters